Cranial Cooling
Cranial Cooling in Contact Sport
“Studying it the right way” — a short- and long-term investigation of acute head cooling
- The question: does cooling the brain early change the course of injury — both near-term recovery and long-term risk?
- Studied “the right way”: prospective and controlled, applied in the acute window, with objective endpoints and clinician governance.
- Two arms — a short-term recovery arm within a season, and a longitudinal arm tracking cumulative burden across a career.
- Device-agnostic: the study tests cooling as an approach, open to any cooling method investigators approve.
- Honest about evidence — early findings are encouraging, not conclusive; the long-term question is named as open.
The question
Does cooling the brain early change the course of injury?
- Short term: does acute cooling reduce symptom burden and shorten recovery after a sports concussion?
- Long term: does reducing acute thermal and metabolic load, across a career, bear on cumulative neurological risk?
Encouraging early evidence exists for the first. The second is open, and answerable only by a long, prospective effort.
What "the right way" means — discipline is the differentiator
Anyone can cool a head. Few would study it like this.
- Prospective and controlled — comparison arms and pre-specified endpoints, not anecdote.
- Applied early — cooling in the acute window, when the mechanism predicts it matters most.
- Objective endpoints — biomarkers, instrumented thermal data, and validated cognitive testing, beyond self-report.
- Clinician-governed — layered onto standard concussion care; clinical judgment governs return-to-play.
- Investigators approve the products — the study tests cooling as an approach, open to any apparatus investigators approve.
- Honest about evidence — claims sized to what is shown; the long question named as unresolved.
Study design — two arms, one investigation
The short arm earns near-term signal; the long arm addresses what matters most.
Short-term — acute recovery, within a season
- Symptom trajectory and recovery time
- Acute injury biomarkers (GFAP, UCH-L1)
- Instrumented thermal data for selected participants
- Comfort, fit, and adherence
Longitudinal — cumulative burden, across a career
- Cumulative head-impact exposure
- Longitudinal axonal-injury marker (NfL)
- Serial cognitive and recovery trajectories
- Long-horizon cohort and brain-donation linkage
A critical design principle — timing is the variable prior work underused
The metabolic cascade begins at impact, so the window for benefit is early.
- The principle. Cooling is mechanistically motivated to be applied as soon as possible after diagnosis, while the metabolic crisis is active, not after it has largely resolved.
- What earlier work missed. At least one study applied cooling roughly 24 hours after diagnosis, well outside the acute window. A delayed-application design can blunt or obscure a real effect, and may undercut its own conclusions.
This study specifies early application by design.
What the originating team brings — a low-cost device engineered to cool heads of all sizes
Thermal engineering and onboard instrumentation, contributed to a device-agnostic study.

- Conformal thermal contact — a proprietary material stack and adjustment system maintain even, effective contact across a wide range of head sizes, the prerequisite for consistent cooling.
- Onboard measurement — garment allows for supplementary sensors to quantify heat load and tissue-temperature signal during use.
- Sideline-practical — non-invasive, closed-loop, and ready within minutes, so early application is operationally feasible and affordable for wide multi-site study.
The material stack — controlled, directional, sustained cooling
Five layers, each doing one job. The stack is what makes the cooling, and the measurement, trustworthy.
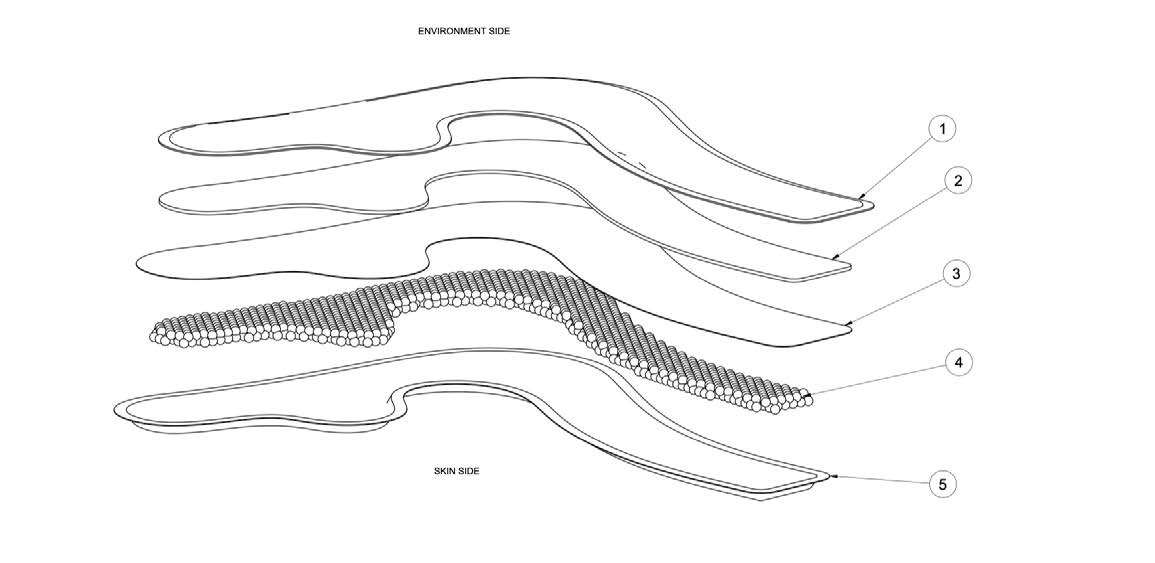
| # | Layer (environment side → skin/head) | Job |
|---|---|---|
| 1 | Outer membrane | Environment-side skin |
| 2 | Foam insulation | Blocks ambient heat |
| 3 | Middle membrane | Separates fill and insulation |
| 4 | Beads + glycerine | Thermal capacity, hold time |
| 5 | Thin skin membrane | Optimal heat transfer |
- Why it works. The skin membrane and beads-glycerine fill deliver and hold cold at the head; the foam insulation forces heat transfer to come from the head, not the surrounding air.
- Why others fall short. Cooling products without insulation or a skin barrier sit too cold against the skin, then are quickly overwhelmed by ambient heat. The result is an uncomfortable spike followed by rapid loss of effect.
Engineering and thermal-performance characteristics; not a claim of clinical effect.
Measurement, in support — objective signals across four layers
How the study stays rigorous. No single layer is sufficient alone.
| Layer | What | How |
|---|---|---|
| Exposure | Impact count and force | Instrumented sensors |
| Acute biomarkers | GFAP, UCH-L1 at the event | Rapid point-of-care assays |
| Longitudinal biomarker | NfL over time | High-sensitivity lab assays |
| Clinical & cognitive | Symptoms, balance, reaction time | Cleared platforms (ImPACT, Sway) |
Sensors and iceless cooling systems allow for a fifth, intrinsic signal: onboard thermal and tissue-temperature data, allowing for measured physics in tandem with efficacy.
The collaboration — different expertise, one protocol
Each role contributes what the others cannot.
- Athletic trainers — first-line observation, early application, comfort and adherence, symptom course.
- Team physicians — clinical judgment, return-to-play, oversight of acute biomarker use.
- Researchers & labs — biomarker analysis, cognitive platforms, longitudinal data and design.
The aim is to answer the question, not to favor a device. Cooling method open to clinical investigators' judgment.
Scientific basis — what the approach is built on
Each element of the design follows from published work (citations below).
- Concussion management is a continuum — recognition, assessment, protection, and graduated return define standard care; the study layers onto it.
- Selective cooling shortened return-to-play — in a head-neck cooling study of ice-hockey players, cooling was associated with faster return.
- A head-neck cooling device is feasible in contact sport — demonstrates that targeted cooling can be delivered practically in the sport setting.
- Early safety and efficacy signal in adolescents — a randomized pilot reported preliminary safety and efficacy after concussion.
- A measurable neurobiological effect — neuroimaging supports a biological effect of selective brain cooling after injury.
Why it matters: the study builds from the successful, on-target selective-cooling literature, not from failed whole-body hypothermia work.
Design rationale · the HALO CTP — built to deploy at scale, and to measure with precision
Two tiers, one approach: an affordable device that makes population-scale study feasible, and an instrumented tier for exacting data.
- Accessible tier — affordable conformal cooling. Material stack and adjustable straps deliver good thermal contact across head sizes, at a low price point. Why it matters: a multi-site, many-athlete, years-long study is only feasible if the intervention is affordable enough to place at high schools, colleges, and the general population.
- Instrumented tier — exacting heat-transfer data. Onboard electronics quantify heat load and tissue-temperature signal, turning the device into an instrument. Why it matters: a smaller instrumented arm validates the mechanism with precision and calibrates what the accessible device delivers at scale.
The HALO CTP is FDA Class I, 510(k)-exempt (21 CFR 890.5700). The study itself admits any clinically accepted cooling method investigators approve.
Gathering the elements — study with us
We are assembling the partners, sites, and instrumentation for a short- and long-term study of cranial cooling in contact sport, designed to be done right. We invite research groups, clinical centers, and longitudinal cohorts to join.
- Patricios JS, et al. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport, Amsterdam, October 2022. Br J Sports Med. 2023;57(11):695-711.
- Gard A, et al. Selective head-neck cooling after concussion shortens return-to-play in ice hockey players. Concussion. 2021;6(2):CNC90.
- Wang H, et al. A Novel Head-Neck Cooling Device for Concussion Injury in Contact Sports. Transl Neurosci. 2015;6(1):20-31.
- Congeni J, et al. Preliminary Safety and Efficacy of Head and Neck Cooling Therapy After Concussion in Adolescent Athletes: A Randomized Pilot Trial. Clin J Sport Med. 2022;32:341-347.
- Walter A, et al. Neurobiological effect of selective brain cooling after concussive injury. Brain Imaging Behav. 2017;12:891-900.